Fat Distribution: Body Fat Types and What Where You Store Fat Means
Fat Distribution: Body Fat Types and What Where You Store Fat Means
You’ve noticed that some people gain weight in their hips and thighs while others build up around the midsection, and you wonder what drives the difference. Fat distribution patterns are largely determined by genetics, sex hormones, and age — but understanding the different types of body fat and what body fat distribution tells you about metabolic health is genuinely useful for both health management and setting realistic expectations. Different types of body fat don’t behave identically, and where you store fat and what it means varies in health significance.
The two most important categories in body fat distribution have very different metabolic implications: subcutaneous fat (under the skin) and visceral fat (surrounding the organs). Knowing which type dominates your pattern changes the urgency and approach of intervention.
Subcutaneous vs Visceral Fat
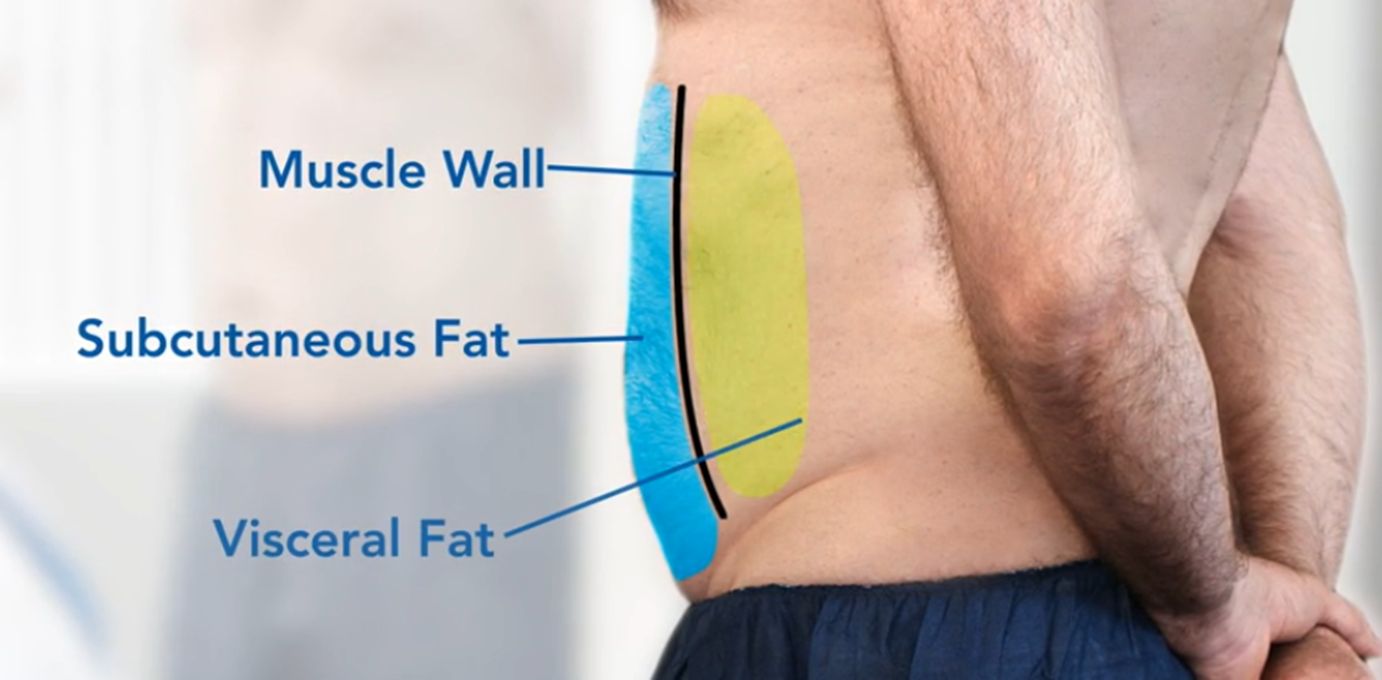
Subcutaneous fat sits directly beneath the skin and is the type you can pinch. It’s found in the hips, thighs, buttocks, arms, and under-belly areas. While subcutaneous fat can be cosmetically concerning, it is metabolically less dangerous than visceral fat — it doesn’t release as many inflammatory cytokines and is less directly linked to cardiovascular disease, insulin resistance, and type 2 diabetes.
Visceral fat surrounds internal organs within the abdominal cavity — around the liver, intestines, and stomach. It’s not visible and can’t be pinched. Visceral fat is metabolically active in a harmful way: it releases free fatty acids directly into the portal vein (which leads to the liver), contributes to chronic inflammation, raises triglyceride levels, and impairs insulin sensitivity. High visceral fat is a stronger predictor of cardiovascular risk than BMI or total body fat percentage.
The Android vs Gynoid Pattern
Android fat distribution (apple-shaped) concentrates fat in the upper body and abdominal region. This pattern is more common in men and post-menopausal women and is associated with higher visceral fat content and greater metabolic risk. Waist circumference is the primary screening measurement: above 40 inches in men and above 35 inches in women indicates elevated visceral fat risk.
Gynoid fat distribution (pear-shaped) concentrates fat in the hips, thighs, and buttocks. This pattern is more common in pre-menopausal women and is largely subcutaneous. Gynoid fat is generally considered less metabolically dangerous than android accumulation, though carrying very high total body fat in any pattern increases health risks. Estrogen promotes gynoid distribution; testosterone and cortisol promote android distribution.
Brown Fat vs White Fat
Among the different body fat types, brown adipose tissue (BAT) and white adipose tissue (WAT) are functionally distinct. White fat is the primary storage form — it stores energy as triglycerides in large lipid droplets. Brown fat is thermogenic — it contains dense mitochondria and generates heat by burning calories rather than storing them. Infants have abundant brown fat; adults retain smaller amounts, primarily around the neck and upper back.
Cold exposure activates brown fat thermogenesis. Regular cold showers, cold water immersion, or cold environments increase the metabolic activity of existing BAT and may promote “browning” of white adipose tissue (creating beige fat). The calorie burn from adult BAT activation is real but modest — estimated at 50 to 100 additional calories per day of cold adaptation in most studies, not the metabolic revolution some claim.
What Fat Distribution Tells You About Health Risk
Waist-to-hip ratio is a more reliable metabolic risk indicator than BMI alone. A ratio above 0.9 in men and 0.85 in women indicates abdominal obesity with elevated cardiovascular and metabolic risk. Waist circumference above 88 cm (35 inches) in women and 102 cm (40 inches) in men is the WHO threshold for high risk. These measurements are cheap, quick, and available to everyone with a tape measure — and they correlate better with metabolic disease risk than weight or BMI in most studies.
Changing Your Fat Distribution
You can’t directly choose where fat is lost from, but visceral fat responds particularly well to sustained aerobic exercise and caloric deficit. Multiple studies show that aerobic training (150+ minutes per week at moderate intensity) reduces visceral fat preferentially compared to subcutaneous fat, even before total body weight changes significantly. This means someone with an android distribution who starts exercising regularly may see waist circumference improvements before the scale changes noticeably.
Dietary patterns associated with lower visceral fat accumulation include Mediterranean-style eating (high in olive oil, fish, vegetables, legumes) and reduced refined carbohydrate and sugar intake. These dietary patterns reduce visceral fat even at the same total calorie intake, suggesting hormonal and inflammatory pathways beyond simple energy balance.
Next Steps
Measure your waist circumference at the natural waist (midpoint between the lowest rib and the iliac crest, relaxed, not sucked in) and calculate your waist-to-hip ratio. Use this as a baseline alongside body weight. If you have an android distribution, prioritize aerobic exercise for visceral fat reduction before or alongside dietary changes. Track waist circumference monthly as a more meaningful health metric than body weight alone.


